Voice care
Cysts, Sulci and Scarring
By Sara Harris, Speech and Language Therapist specialised in Voice Disorders.
Cysts
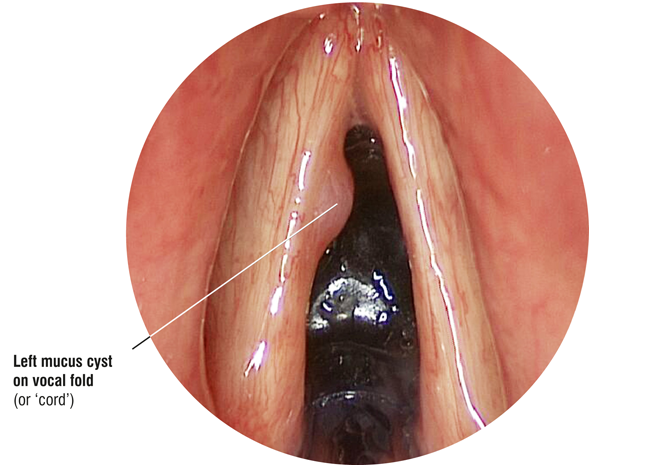
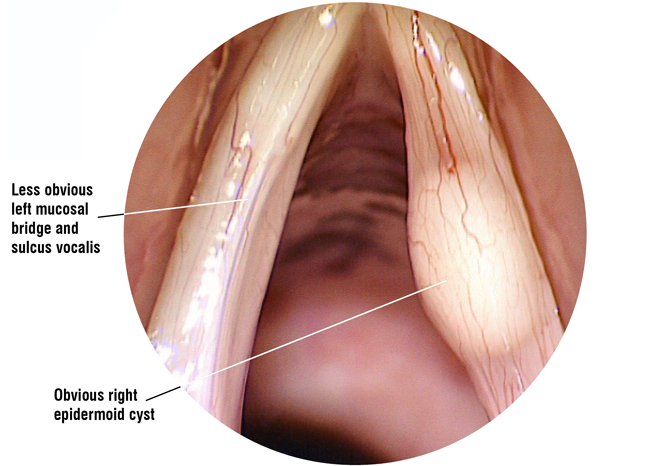
There are basically two types of cyst that can occur on the vocal folds (often referred to as ‘vocal cords’). Probably the most common is the retention cyst, which develops when the duct of a small mucus producing gland becomes blocked forming a closed sac that fills with fluid or a semi-solid material. The origins of other cysts, known as epidermoid cysts, that appear inside the layers of the vocal fold are less well understood. They tend to be more solid in nature than retention cysts and they are usually long standing, possibly even congenital. Often they are more difficult to spot without specialist equipment as they are not necessarily visible with routine examination techniques. Patients with epidermoid cysts often report that they have always had a deeper than average voice, even as a child. However, they may not be aware of any real vocal difficulties until the vocal load is increased should they, for example, become a singer, actor or teacher. Occasionally a cyst will burst, discharging its contents but leaving a small strip of remnant mucous membrane (vocal fold lining) that was once part of the cyst roof. These are referred to as mucosal bridges. Unfortunately, beneath them usually lies the scarred floor of the cyst, which is deeply adherent to the underlying ligament, leaving an area of vocal fold that cannot vibrate.
Sulci
A sulcus (plural sulci) is a small groove or furrow that creates a depression along part of the vocal fold. These again may form congenitally, but some may develop when cysts rupture leaving a small pit. The pit then elongates over time with repeated vibration of the vocal fold. Sulci can vary in length. Some are very short while others are almost as long as the vocal fold itself. Most small sulci are very difficult to spot at examination and do not trouble the average voice user. However, for professional voice users, they may interrupt the vocal fold vibration at certain pitches, causing the voice to cut out or become pitch unstable.
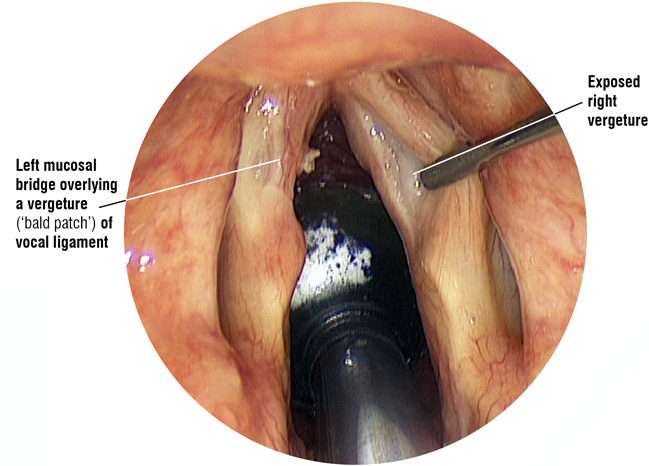
Vergetures
Occasionally, a laryngologist may diagnose a “vergeture”. A vergeture is a defect in the layered structure of vocal fold (see the diagram below) where the pliable outer layer is missing over a small area of the vocal fold, rather like a bald patch on a tyre. It appears very similar to a sulcus at examination and has similar effects on vocal fold vibration.
Scarring
Scarring occurs when fibrous tissue is laid down to repair damage to a vocal fold. Scarring is a normal part of the healing process, but it tends to knit the vocal layers together with stiff fibrous tissue. Excessive scarring can develop as the result of repeated injury from poor or abusive voice use, in response to surgery or to some other form of vocal fold injury such as bleeding or irritation from inhaled noxious substances.
Cysts, sulci and scars can all vary in size and extent. Their size and extent will determine how much of the vocal fold is affected and how seriously vocal fold vibration is impaired. The bigger the defect, the greater the effect it will have on voicing and the more difficult it will be to treat effectively.
The Secret is in the Structure
The key to understanding why vocal fold problems such as cysts, sulci, vergetures, mucosal bridges and scarring (often referred to as vocal fold lesions) are so difficult to deal with lies in the complex structure of the vocal folds.
Each vocal fold is a layered structure, the outer layers of which are pliable, deformable and designed to slide smoothly over the deeper layers during voicing.
A flexible mucus membrane forms the outer covering of the vocal fold (the epithelium). Beneath are several layers of connective tissue (the lamina propria). The outer (superficial) layer of the lamina propria is gelatinous in nature and separates the mucous membrane (epithelial) outer cover from the stiffer underlying vocal ligament. Beneath the ligament lies the vocalis muscle.
(Just to confuse things, you may read literature that refers to the vocal fold "cover" and "body", where the cover is considered to include the epithelium and the superficial (gelatinous) layer of the lamina propria, while the body includes the stiffer ligament and underlying muscle. This text however refers to the epithelium as the "outer covering" of the vocal fold and it should not be confused with the idea of "cover" described above).
The epithelium is exposed to a considerable upwards force as the air rushes between the vocal folds during voicing. The gelatinous layer of the lamina propria cushions the epithelium by allowing it to slide upwards and outwards in response to the air pressure. This upward and outward movement of the epithelium is visible when the vocal folds are examined under stroboscopic light appearing like waves rippling over the upper surface of the vocal fold. The movement is known as the mucosal wave. A clear voice quality depends on whether or not the vocal folds can generate normal mucosal waves. Any condition that "tethers" the epithelial cover to the underlying ligament will disrupt or reduce the mucosal wave. The vocal folds will no longer vibrate over the affected area and the voice quality may be altered. Cysts, sulci, vergetures and scarring all either disrupt these layers by tethering them together or affect voicing because small areas of the epithelium and lamina propria are absent.
What are the symptoms of cysts, sulci and scarring?
The symptoms you might notice if you have any of these lesions might include some or all of the following:
- Breaks in voicing across specific areas of the vocal range
- Difficulties initiating voicing (slow onset) and in sustaining voicing to the end of a sentence (early offset)
- The difficulties initiating voicing also sometimes occur following unvoiced (whispered) consonants in a sentence
- A rough, hoarse, often harsh vocal quality
- A feeling of strain and of having to ‘push’ to keep the voice going
- If the vocal folds are very stiff because the lesion is more extensive, the pitch of the voice may rise and be combined with a strained, rough quality.
How can I tell if I have a cyst, sulcus or scar?
Unfortunately all these symptoms can also occur in other vocal conditions, so it is very important to seek diagnosis from a voice specialist ENT surgeon (laryngologist), preferably one working in a multidisciplinary voice clinic.
The laryngologist will need to examine your vocal folds with specialist equipment, such as stroboscopy or high speed photography, in order to identify any areas of vocal fold stiffness that might indicate the presence of a cyst, sulcus or scar. Without this special equipment these lesions may be difficult to identify. Even when good equipment is available, it still may not always be possible to determine exactly what is causing a stiff area until the vocal folds can be palpated and examined under a microscope during surgery. There is good research evidence to show that the diagnosis made in a general outpatient clinic may change or be extended when a patient is seen with specialist equipment in a voice clinic (1, 2, 3, 4).
Can these lesions be treated conservatively?
Patients with identifiable cysts or extensive scarring will usually require surgery with follow up speech therapy to try and reduce the chance of post operative scarring. Where the area of stiffness is small, as in the case of minor sulci or minimal scarring, conservative treatment in the form of speech therapy, laryngeal manipulation and singing lessons may be tried initially. These methods of treating the voice may well improve the vocal quality, comfort and stamina by reducing the strain caused by excessive muscle tension and constriction that develop in compensation for the increased vocal stiffness. To some extent, good voice production may also help to shake loose stiffness and scarring but its effect will be limited.
If conservative treatment fails to resolve the symptoms these lesions will require surgery.
Surgery
Recent advances in surgical technique (phonosurgery) mean that cysts and some sulci can be removed and scars can be modified, either resolving or improving the vocal symptoms. It is important to choose a voice specialist laryngologist who is familiar with phonosurgical techniques and who will understand the needs of professional voice users.
Your surgeon will explain your diagnosis and discuss, as honestly as they can, what they plan to do at surgery and the possible outcomes. Unfortunately, examination in the voice clinic, even with specialist equipment, may only tell the surgeon that there is an area of vocal fold stiffness. It will not necessarily determine what is causing it. The nature of the problem and its full extent may only be discovered at the time of surgery, making it very difficult for the surgeon to be accurate in either the outpatient diagnosis or outcome prognosis.
Many surgeons will refer you to speech therapy at the time you are placed on the waiting list for surgery. It is important that you make contact with the therapist as soon as you know your surgery date so that they can arrange a timely appointment for you. Usually, the sooner you receive therapy the faster you can begin to develop good vocal technique again. The aim of post operative voice therapy is to resolve any remaining compensatory muscle tension and to shake loose stiffness that is a normal part of post operative healing.
Are the results of surgery good?
Cysts frequently respond well to surgical removal and the results are generally good. Occasionally they can recur, so it is important to attend a review appointment with your laryngologist and to return and see them again should your symptoms recur.
Sulci can sometimes be removed. The results are more variable as some of the pliable lamina propria layers may be absent or scarred down in the area of the sulcus making surgery more challenging.
Scarring can be more difficult to remove and the results are therefore less predictable. Most people, however, report vocal improvement following surgery.
It is important to remember that recovery after removal of these lesions takes longer than simple healing. Do not be alarmed if your voice sounds temporarily worse after surgery. This should resolve with voice therapy over time and most people see good improvement within three months. It is not uncommon, however, to see continuing improvement for six months to a year or more.
If you are diagnosed with a cyst, scar or a sulcus, do not despair. Phonosurgery techniques have made it possible to treat these disorders successfully most of the time and, with voice therapy, you are very likely to make a good recovery. The journey back from these problems will inevitably take longer than you would like, but it is usually well worthwhile.
Author Sara Harris with acknowledgements to Tony Aymat, Nick Gibbins, Tom Harris and John Rubin.
References:
- Report on the British Voice Association World Voice Day Questionnaire for Voice Clinics presented at Voice Clinics Forum, November 2012.
- Does a specialist voice clinic change the ENT clinic diagnosis? Phillips, P.S. et al, Logopedics, Phoniatrics ,Vocology: 2005 Vol. 30: pp 90-93.
- Diagnostic Value of Stroboscopic Examination in Hoarse patients. Woo, P. et al, Journal of Voice, 1991 Vol. 5, No 3: pp 231-238.
- From Voice Clinic to Theatre: What are we not seeing? Awad, R et al, Paper accepted for the 11th Congress of the European Laryngological Society, Genoa, Italy, 8-11th June, 2016.
This information is intended for guidance purposes only and is in no way intended to replace professional clinical advice by a qualified practitioner.
 Join us Now!
Join us Now! our newsletter
our newsletter free voice care leaflets & information – download here
free voice care leaflets & information – download here Help our work by donating while you shop
Help our work by donating while you shop