Voice care
Muscle Tension Dysphonia (MTD)
Sara Harris, Voice Specialist Speech and Language Therapist, Team Member, Lewisham Voice Clinic, London and Sara Caldwell, Voice Specialist Speech and Language Therapist, Cheshire.
Effective, comfortable speech and singing relies on maintaining a comfortable balance of tension between the muscles of voicing. Certain muscles were designed to be the primary movers in voicing and can stand up to the workload we give them. These include the muscles of the vocal folds themselves as well as the muscles that control vocal fold closure, pitch change and resonance balance in the upper airway above the larynx. If these muscles become overly tight, or alternatively are underused, other, less effective muscles around the larynx are recruited to ‘help out’. These recruited muscles were not usually designed to be primarily involved in voicing so over time, the system tires and the voice begins to produce audible symptoms. It may start to sound hoarse, tight, constricted and unreliable. The pitch may become too high, too low, unstable or yodelling. The voice often starts to feel strained too. It may be effortful to produce and discomfort or even pain can develop, particularly with heavy voice use or when speaking against background noise. When this happens it is usually referred to as a Muscle Tension Dysphonia or MTD.
In most cases, MTD produces these vocal symptoms without any actual physical damage. However, if the voice continues to be used habitually in this way over the longer term MTD can sometimes cause physical changes. Usually the changes start with soft vocal fold swelling, often accompanied by dryness and general laryngeal irritation. If the damaging vocal habits continue long enough the swelling can progress so that the vocal folds become stiffer and fibrous tissue develops in response to the repetitive injury. It is therefore important that any hoarseness is investigated by a laryngologist early to exclude more serious causes and prevent physical changes developing.
Although Muscle Tension Dysphonia is the most common name we give to voice disorders that develop as a result of the way in which the voice is habitually used, they have been given many other names and classifications in the past. Some others you may come across include ‘Functional Dysphonia’, ‘Vocal Hyperfunction’, ‘Muscle Misuse Dysphonia’ and ‘Muscle Imbalance Dysphonia’. What they all share in common is that they are associated with inappropriate muscle use within the larynx during voicing. Although normally MTD is associated with constriction and too much muscle effort (hyperfunction), it can also apply to vocal postures where there appears to be too little muscle effort in the vocal folds causing weakness and bowing (hypofunction). In these cases, the excess muscular effort is occurring in other, less effective muscles in and around the larynx.
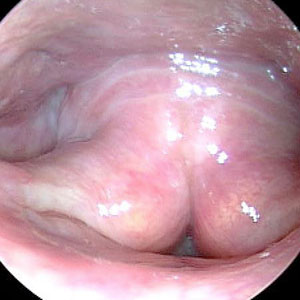
Clinicians will often subdivide MTD cases into recognised patterns of vocal posture. For example, ‘MTD with lateral compression’, where the vocal folds appear long and stretched and the false vocal folds/side walls of the larynx appear to be pulled inwards towards the midline (note that in the photograph the true vocal fold edges are not completely straight and appear ‘bowed’).
The false vocal folds may even obscure the view of the true vocal folds in extreme versions of this vocal posture (sometimes referred to as ‘dysphonia ventricularis plicae’ in the medical literature).
The larynx may also constrict from the back towards the front so that the arytenoid cartilages (that hold the back or posterior ends of the vocal folds) appear pulled forward obscuring some or all of the vocal folds (postero-anterior [PA] constriction).
Alternatively, the epiglottis (or its base) which lies at the front of the larynx appears pushed backwards obscuring the front/mid portion of the vocal folds (antero-posterior [AP] constriction) allowing the cuneiform cartilages to tilt backwards.
To complicate the picture further, MTD can co-exist with or develop in response to laryngeal pathology. For example, false fold constriction and lateral compression frequently occur as compensations for a weak or paralysed vocal fold or where there is a small scar, sulcus or vergeture on the vocal fold[1]. It is therefore important for the larynx to be properly examined and any structural abnormality excluded before a diagnosis of MTD can be made.
In the early 1980s, Morrison and Rammage[2] described another common pattern of muscle misuse where the first two thirds of the vocal folds are firmly closed but the posterior portion (back end) remains held widely open. Initially, they termed this posture ‘Muscular Tension Dysphonia’ but later changed it to ‘Laryngeal Isometric Disorder’. It is easy to see with all the terms used in voice clinics, in the literature and in medical correspondence why patients can become very confused about their diagnosis, especially when given a copy of the letter sent from their laryngologist to the referring GP. The most important thing to remember from the patient’s point of view is that all these terms basically amount to the same thing: that the hoarseness is being created not by any vocal disease or damage, but by the way in which the laryngeal muscles are being used. While each person may be using a different pattern, the voice clinic team will be able to identify and explain what is happening and arrange the treatment most likely to resolve the problem.
What are the symptoms of Muscle Tension Dysphonia?

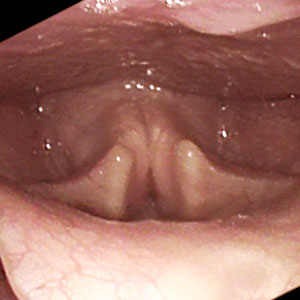
Normal gesture during phonation
Image courtesy Tom Harris

MTD with Lateral Compression
Image courtesy Tom Harris

Dysphonia Plicae Ventricularis
Image courtesy Tony Aymat
MTD Postero-Anterior Collapse
Image courtesy Tom Harris
MTD Antero-Posterior Compression
Image courtesy Nick Gibbins

Laryngeal Isometric Disorder
Image courtesy Tom Harris
There are many symptoms of MTD and they can vary both within the same person and between individuals. They can also come and go so that sometimes the voice is normal, then for no apparent reason the hoarseness and discomfort return.
Some of the symptoms to watch out for include changes in voice quality, particularly during long periods of voice use or at the end of the day. The voice may start to sound:
- Rough, hoarse or develop a raspy quality
- Tight, tense, strained with a constricted or 'squeezed' quality
- Breathy, weak and quiet, fading out towards the end of sentences
- Intermittent with voice 'breaks' where the sound cuts out briefly or where voice is slow to start vibrating
- Too high or low in pitch, or the pitch may be unstable
Changes in sensation when speaking or singing may occur including:
- Tiredness, aching or pain especially when speaking/singing loudly against noise or for long periods
- Dryness or scratchiness
- A sense that talking is effortful and hard work
There may be changes in vocal stamina in that we can no longer talk or sing for as long as we used to without one or more of the above symptoms developing. This may be quite a small change, such as mild vocal tiredness towards the end of a busy day, or it may be severe, with symptoms developing after only ten minutes of voice use.
How is Muscle Tension Dysphonia diagnosed?
MTD can only be diagnosed through examination of the larynx. Ideally an ear, nose and throat doctor (ENT Surgeon/Laryngologist) and a speech and language therapist (SLT) working together in a voice clinic would investigate the causes of your voice problem through observation of the larynx during voice production. A careful history will be taken to identify any other health or lifestyle problems that might be causing or contributing to the MTD. It is important that any contributing factors are identified and treated before voice therapy is started.
They will also analyse how the voice is being produced and record how it sounds to monitor treatment.
What causes Muscle Tension Dysphonia?
There are usually a number of factors involved in the development of a MTD. The most common ones include:
- Long-term patterns of ineffective voice use
- Sudden changes in voice production associated with a period of vocal overuse, an infection or emotional stress
- Compensation for an underlying vocal fold problem such as a cyst, paresis, or fatigue in the vocal muscles
- A 'guarding' response to acid reflux or some other irritant
- A combination of some or all of the above factors
How is Muscle Tension Dysphonia treated?
Depending on the diagnosis, MTD without any other vocal fold abnormality is usually treated by a SLT specializing in voice disorders. Treatment may require only a few sessions or may take several months depending on how long the problem has been present and the individual’s response to treatment. The goal of voice therapy is to decrease excessive or inappropriately placed laryngeal tension so that the vocal muscles can function effectively again.
If MTD is the primary cause of damage to the vocal fold, or alternatively, has developed to compensate for an underlying vocal or health problem, the ENT surgeon will explain and discuss the medical/surgical treatment options available. If surgery is required it is important to attend voice therapy during your recovery to resolve any persisting symptoms of MTD that might undermine the improvements surgery has provided.
What does Voice Therapy involve?
The SLT will help you explore how you use your voice and identify any problem vocal behaviours or lifestyle factors contributing to your voice disorder. Your therapist will use a range of approaches to help you find a more effective way to produce your voice when speaking and/or singing. These may include:
- Working on your posture
- Improving your breathing pattern to support the voice
- Relaxation techniques to reduce the general neck/shoulder tension that contributes to vocal tension
- Specific vocal exercises designed to redistribute the working load to the appropriate vocal muscles
- Laryngeal massage to reduce tension in the throat and laryngeal muscles
What can I do to help prevent or resolve Muscle Tension Dysphonia?
You can help improve the symptoms of MTD, or reduce the chances of it developing, by maintaining good vocal care and in particular by avoiding the following:
- Yelling and screaming
- Speaking/singing excessively loudly, especially against noise
- Speaking/singing outside your own comfortable pitch range
- Speaking/singing with excessive tension/constriction in the vocal muscles
- Speaking/singing when out of breath or without good breath support
- Speaking with a hard glottal attack
- Excessive coughing and throat clearing
- Whispering or trying to protect the voice
Will I always have the condition/need treatment?
Reducing general sources of tension and stress in your everyday life, observing good voice care and following the advice you receive during voice therapy will help you maintain the improvements you have made and reduce the likelihood of MTD recurring.
This information is intended for guidance purposes only and is in no way intended to replace professional clinical advice by a qualified practitioner.
References
Koufman, JA, Evaluation of Laryngeal Biomechanics by Transnasal Flexible Laryngoscopy. In: Diagnosis and Treatment of Voice Disorders, 4th Edition. Editors: Rubin, JS, Sataloff, RT, and Korovin, GK, 2014, Plural Publishers, San Diego, California. (In press)
Morrison, M and Rammage, L. The Management of Voice Disorders, (1994) Singular Publishing Group Inc. San Diego, California.
Acknowledgements
With thanks to John Rubin, F.R.C.S. Tom Harris, F.R.C.S and Jackie Ellis for help with editing and to Tom Harris, F.R.C.S., Nick Gibbins, F.R.C.S. and Tony Aymat, F.R.C.S. for the photographs.
 Join us Now!
Join us Now! our newsletter
our newsletter free voice care leaflets & information – download here
free voice care leaflets & information – download here Help our work by donating while you shop
Help our work by donating while you shop